JAMIE L. WAGNER, PHARMSD, BCPS
INFLUENZA VACCINE TYPES
The influenza vaccine can be produced in 3 different ways; as an egg-based, cell-based, or recombinant formulation.3,4 Egg-based manufacturing relies on replicating live flu virus inside fertilized hen eggs before extracting, inactivating or weakening, and purifying it for vaccine production.3 This process can be both resource-and time-intensive.5 Additionally, egg-adapted changes to the virus may occur, causing a decrease in effective antibodies against the virus.4
Cell-based manufacturing relies on replicating live flu virus inside Madin-Darby canine kidney (MDCK) cells. This egg-free process results in faster production time, reduces egg-adapted viral changes,4 and allows cells to be cryopre- served, reconstituted, and scaled up at any time.5 In addition, the MDCK cells are easily manipulated from both a biological and manufacturing perspective, further enhancing the ease of viral production.5 At this time, only 1 egg-free influenza vaccine is produced in this manner and approved by the FDA for use during the 2019-2020 flu season.4
Recombinant technology combines influenza hemagglutinin DNA with a nonhuman virus into 1 recombinant virus. The virus is then introduced into a specified cell line in a lab, allowing for rapid production of a hemagglutinin antigen3 to be collected and purified for market as a recombinant vaccine. To date, only 1 influenza vaccine is produced in this manner and approved by the FDA for use in the United States.
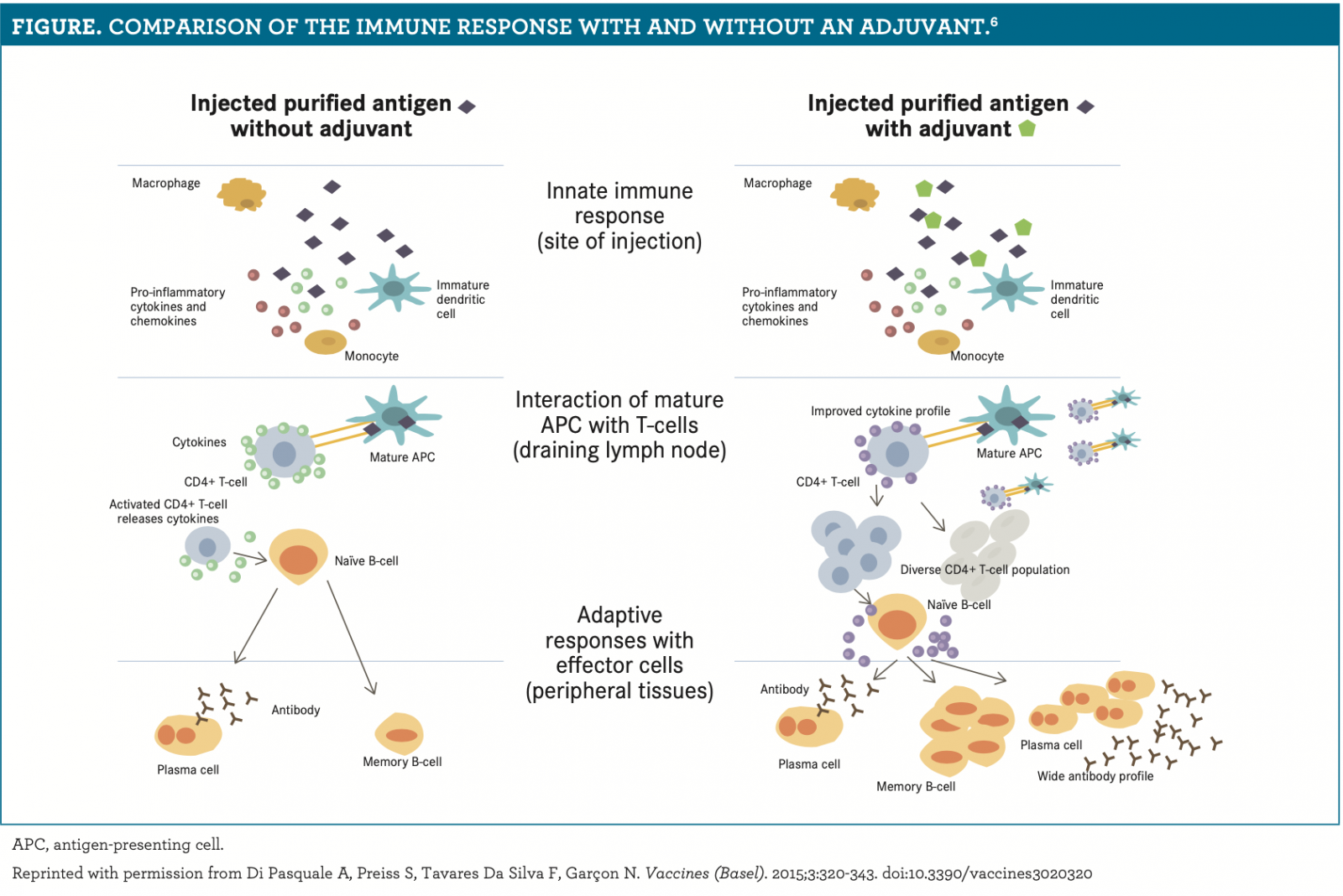
In 2016, the influenza vaccine was combined with an adjuvant, MF59, an oil-in-water emulsion composed of a naturally occurring oil (squalene).4-6 MF59 enhances the immune response by inducing higher antibody titers than nonadjuvanted formulations, generating cross-reactive antibodies, and eliciting an immune response similar to a natural innate response (figure ).6 Using MF59 in the influenza vaccine reduces the amount of viral antigen contained within each dose and the number of doses required.6,7
INACTIVATED VS LIVE INFLUENZA VACCINES
Most influenza vaccines contain inactivated viral proteins. A live virus is chemically inactivated and then treated with a detergent to expose all the viral proteins.5 Inactivated virus within the vaccine cannot replicate or cause disease, even if a patient is immunocompromised; therefore, an inactivated influenza vaccine can be administered to all patients who are at least 6 months of age.8
The live, attenuated influenza virus is designed to induce both humoral and cellular immunity5 through replication in the nasopharynx.1 The virus is specifically modified to restrict the reaction, pathogenicity, and replication in the lower respiratory tract, and permit replication to the nasopharynx.1 Because the virus is still able to replicate, its use is not recommended in children with asthma, patients with a compromised immune system caused by medications or HIV infection, close contacts/caregivers of immunocompromised patients, and patients who are pregnant.9
MATCHING THE VACCINE TYPE TO MEET PATIENT NEEDS
Certain vaccine types are recommended for patient populations who are at increased risk of complications from influenza infection.
Patients who are over the age of 65 are at higher risk of influenza complications, including hospitalization and death, because the immune system tends to wane in its ability to mount an effective response against an invader.10 Indeed, about 54% to 70% of seasonal influenza-related hospitalizations and 70% to 85% of seasonal influenza-related deaths occur in patients who are 65 years and older.7
Three ways to combat the waning immunity are to increase the amount of antigen in the vaccine (“high-dose”), include an adjuvant with the standard dose (eg, MF59), or administer a recombinant vaccine.2,11
The CDC’s Advisory Committee on Immunization Practices (ACIP) recommended that patients over the age of 65 receive any of the age-appropriate inactivated or recombinant influenza vaccines. Although ACIP does not recommend a spe- cific type of vaccine over another, the 2 inactivated, trivalent vaccines specifically recommended for patients over the age of 65 include the high-dose vaccine and the adjuvanted standard-dose vaccine.2
Specific populations are at an increased risk of severe illness and complications from influenza due to either an immature immune system or a reduced vaccine response.6 These include patients with any chronic disease or an immunocompromised state, those who are pregnant, those aged 6 to 59 months, and those with allergies to egg or latex.2,12
For patients with any chronic disease (eg, pulmonary, cardiovascular [excluding isolated hypertension], renal, hepatic, neurologic, hematologic, or metabolic [including diabetes mellitus]), ACIP recommends prioritizing an age-appropriate, inactivated or recombinant influenza vaccine over a live, attenuated influenza vaccine.2
Patients with immunocompromising conditions should receive any age-appropriate, inactivated or recombinant influenza vaccine and not the live, attenuated vaccine.2 Similarly, pregnant or postpartum women should receive any age-appropriate, inactivated or recombinant vaccine rather than the live, attenuated vaccine.2
For children aged 6 to 59 months, ACIP recommends administering 2 doses of an age-appropriate, inactivated influenza vaccine at least 4 weeks apart during their first influenza season.2
For patients with egg allergies, there are 2 inactivated, quadrivalent influenza vaccines available: the recombinant vaccine and the cell culture–based vaccine. However, unless a patient experienced a severe allergic reaction after prior influenza vaccine administration, ACIP recommends that all persons with a history of egg allergy still receive an annual, age-appropriate vaccine.2
As of the 2019-2020 influenza season, no influenza vaccines, vials, or syringes contain latex.12
The use of monoclonal antibodies to treat influenza is still under investigation. One example is VIS410, a broadly neutral- izing IgG1 monoclonal antibody with activity against influenza strains containing H1, H3, H5, and H7 subtypes. A phase 2 trial comparing a single infusion of VIS410 to placebo in nonhospitalized patients with uncomplicated influenza infection demonstrated a reduction in viral replication and reduction-in-symptom score by day 3 post treatment.13 Further evaluation on the timing and dosing of this drug is needed before broad recommendations can be made.
Understanding the different types of vaccines that are available in the United States, as well as the recommended use for each in appropriate patient populations, will ensure positive patient outcomes. Pharmacists are in a prime position to recommend the most appropriate influenza vaccine when taking into account the patient’s age, allergies, and comorbid conditions.
REFERENCES
- Background document for “Prevention and Control of Seasonal Influenza with Vaccines: Recommendations of the Advisory Committee on Immunization Practices—United States, 2019-20 Influenza Season.” CDC. Updated September 10, 2019. Accessed June 4, 2020. https://ift.tt/2CFTNGU
- Grohskopf LA, Alyanak E, Broder KR, Walter EB, Fry AM, Jernigan DB. Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices–United States, 2019-20 influ- enza season. MMWR Recomm Rep. 2019;68(3):1-21. doi:10.15585/mmwr.rr6803a1
- How influenza (flu) vaccines are made. CDC. Updated December 12, 2019. Accessed June 4, 2020. https://ift.tt/2OQQkrr
- Cell-based flu vaccines. CDC. Updated October 11, 2019. Accessed June 4, 2020. https://ift.tt/3hvlUXY
- Wong SS, Webby RJ. Traditional and new influenza vaccines. Clin Microbiol Rev. 2013;26(3):476-492. doi:10.1128/CMR.00097-12
- Di Pasquale A, Preiss S, Tavares Da Silva F, Garçon N. Vaccine adju- vants: from 1920 to 2015 and beyond. Vaccines (Basel). 2015;3(2):320-343. doi:10.3390/vaccines3020320
- Flu vaccine with adjuvant. CDC. Updated September 4, 2019. Accessed June 4, 2020. https://ift.tt/2CWyKj8
- Key facts about seasonal flu vaccine. CDC. Updated April 28, 2020. Accessed June 4, 2020. https://ift.tt/2n8ZqVK
- Live attenuated influenza vaccine [LAIV] (the nasal spray flu vaccine). CDC. Updated November 7, 2019. Accessed June 4, 2020. https://ift.tt/2cOnPZf prevent/nasalspray.htm
- People 65 years and older & influenza. CDC. Updated November 21, 2019. Accessed June 4, 2020. https://ift.tt/2TeQSKs
- Houser K, Subbarao K. Influenza vaccines: challenges and solutions. Cell Host Microbe. 2015;17(3):295-300. doi:10.1016/j.chom.2015.02.012
- Influenza vaccines—United States, 2019–20 influenza season. CDC. Updated August 22, 2019. Accessed June 4, 2020. https://ift.tt/2ZTxSEX vaccines.htm
- Hershberger E, Sloan S, Narayan K, et al. Safety and efficacy of monoclonal antibody VIS410 in adults with uncomplicated influenza A infection: results from a randomized, double-blind, phase-2, placebo-controlled study. EBioMedicine. 2019;40:574-582. doi:10.1016/j.ebiom.2018.12.051
"type" - Google News
July 23, 2020 at 07:10PM
https://ift.tt/39lNcxj
Influenza Vaccine–Type Differentiation Updates for 2020 - Pharmacy Times
"type" - Google News
https://ift.tt/2WhN8Zg
https://ift.tt/2YrjQdq
Bagikan Berita Ini














0 Response to "Influenza Vaccine–Type Differentiation Updates for 2020 - Pharmacy Times"
Post a Comment